The value of a personal injury claim is not determined by injury severity alone. It is determined by how clearly that injury is documented, structured, and linked to the incident in question.
Case valuation depends on whether medical evidence forms a coherent, chronological record that establishes causation, the necessity of treatment, and measurable impact. When medical data is fragmented across providers and facilities, it creates evidentiary gaps that insurance adjusters routinely leverage to suppress settlement offers.
Effective medical record organization for PI cases converts raw clinical data into a defensible legal framework. It aligns diagnostic findings, treatment progression, and functional limitations into a structured timeline that supports damage modeling.
By centralizing and sequencing documentation, legal teams reduce valuation ambiguity and limit opportunities for defense challenges. In high-exposure litigation, structured records are not administrative tools; they are valuation drivers.
Establishing the Causal Link Through Documentation
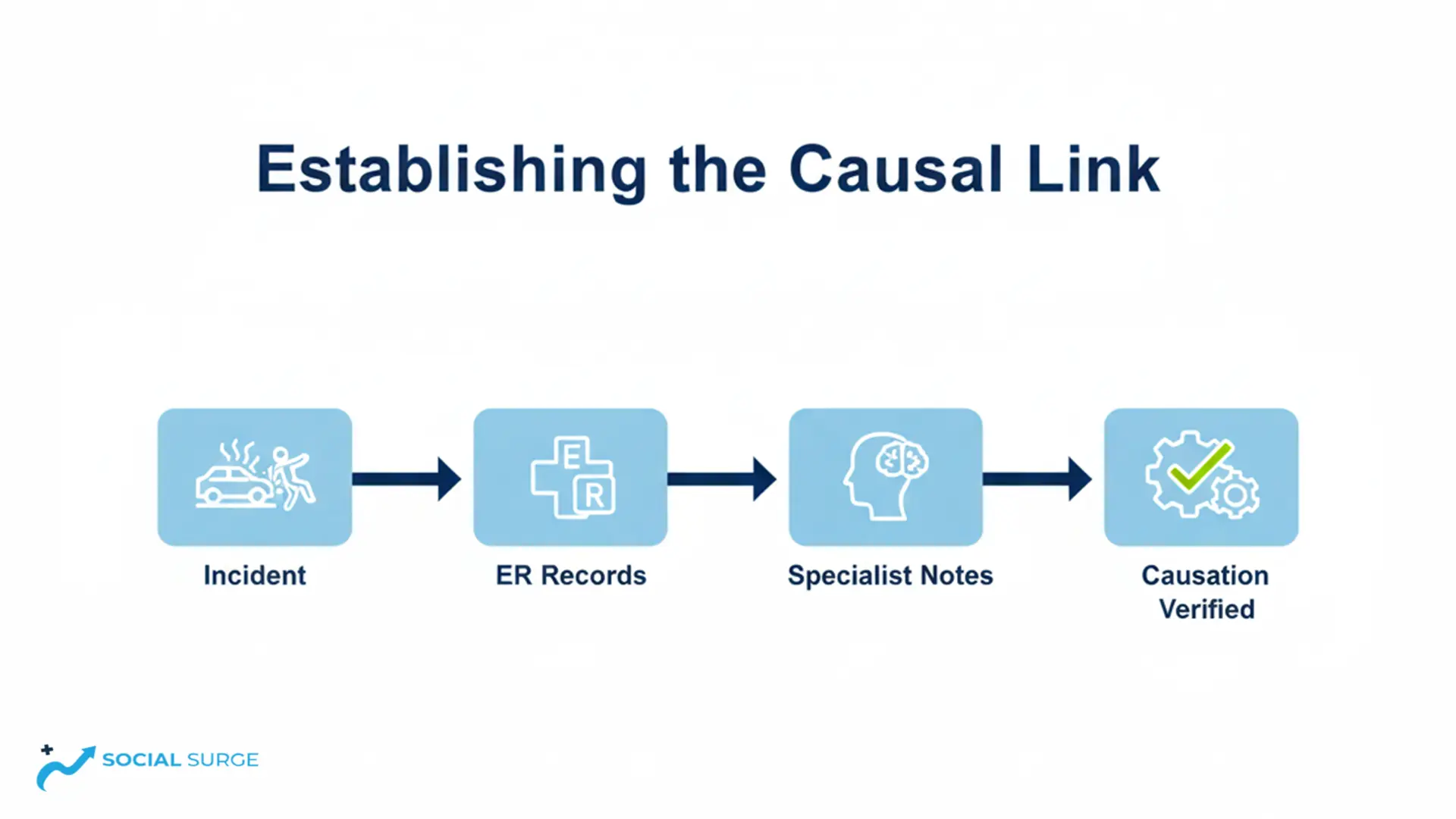
Medical documentation in personal injury claims establishes the evidentiary baseline for causation. Emergency and hospital records created immediately after an incident carry heightened probative value because they capture symptoms, mechanism of injury, and initial clinical impressions before claim strategy develops. These entries anchor the timeline and define whether the injury can be directly attributed to the triggering event. In the absence of contemporaneous documentation, defense counsel can attribute symptoms to intervening causes or pre-existing degeneration.
The durability of a claim often depends on the precision of these early notes. Courts and insurers rely on licensed providers because contemporaneous clinical observations carry greater evidentiary weight than retrospective testimony. Specific entries regarding the mechanism of injury, objective findings, and functional limitation strengthen causation analysis under standard evidentiary review, including in jurisdictions applying stricter scrutiny to aggravation claims. Clear documentation at intake frequently determines whether liability disputes escalate or resolve early.
Treatment continuity further reinforces credibility. When follow-up visits reflect a consistent progression of symptoms, the medical timeline becomes internally coherent. Inconsistent reporting, unexplained symptom escalation, or documentation gaps, however, create leverage for defense arguments. Structured review of each encounter ensures that the causation narrative remains aligned with clinical evidence rather than undermined by avoidable inconsistencies.
Analytical Review: Case Valuation Mechanics
The impact of medical records on settlement value is most evident in the distinction between subjective symptom reporting and objective clinical evidence. Insurers apply greater weight to diagnostic imaging, quantified range-of-motion deficits, surgical findings, and documented neurological impairment than to generalized pain complaints. When records are structured to highlight these objective markers, valuation models reflect higher severity coding. Disorganized files, by contrast, dilute high-value findings within routine administrative documentation, reducing perceived claim strength.
Chronological structure also influences how the impact of medical records on settlement value is calculated over time. A consistent progression from acute injury to documented functional limitation supports both economic and non-economic damages. Clear treatment sequencing demonstrates medical necessity, duration of impairment, and resistance to conservative care. Without this structure, adjusters may classify care as excessive or unrelated, directly suppressing projected damages.
Understanding how medical records affect case valuation requires attention to forward-looking documentation. Functional capacity assessments, permanency ratings, and specialist projections establish the foundation for future medical expense and loss of earning capacity calculations. When these elements are explicitly integrated into the treatment timeline, the damages model becomes evidence-driven rather than assumption-based. This alignment between clinical findings and financial projections reduces negotiation volatility and strengthens settlement positioning.
Navigating Insurance Adjuster Review Behavior
Insurance evaluators follow a systematic review protocol to identify weaknesses in a claim. They focus on treatment gaps, missed appointments, and inconsistencies between accident reports and later specialist notes. Fragmented or poorly organized files allow adjusters to argue that care was unnecessary, symptoms are exaggerated, or damages were not mitigated.
Beyond the records themselves, adjusters cross-check medical notes against social media activity, employment records, or other external data. Any contradiction, such as a normal range of motion documented while a claimant reports total disability, can sharply reduce settlement projections. This underscores the critical importance of contemporaneous, accurate documentation for every visit.
Structured Comparison: Disorganized vs. Structured Files
- Disorganized File: Multiple providers with fragmented records; unexplained treatment gaps; objective findings buried in administrative notes; inconsistent symptom reporting; delayed access to operative reports.
- Structured File: Complete longitudinal timeline; interruptions explained; high-value imaging prioritized; continuity of symptom progression verified; attorney-ready indexing enables rapid strategic review.
Countering Defense Tactics Through Organization
Implementing medical record organization for PI cases is the most effective defense against adjuster scrutiny. Centralized review enables the legal team to identify and resolve documentation gaps before mediation or deposition. Coordinating with licensed medical professionals ensures the file accurately reflects the complete clinical narrative, strengthening causation and treatment continuity. Professional medical record review services shift a firm from reactive case handling to a proactive, litigation-ready strategy.
Settlement value is further preserved when pre-existing conditions are transparently documented. Rather than concealing prior injuries, a structured record differentiates old issues from new trauma through comparative imaging and explicit aggravation statements. This prevents defense counsel from devaluing claims by misclassifying injuries as chronic or unrelated, a distinction often required under Texas law to support aggravation recovery.
Common Defense Tactics to Monitor
- The Gap Tactic: Exploiting treatment interruptions to argue medical improvement.
- Baseline Distortion: Attributing current symptoms to prior asymptomatic findings.
- Subjectivity Dismissal: Discounting pain reports that lack immediate diagnostic confirmation.
- Mitigation Defense: Citing missed appointments to reduce non-economic damages.
- Contradiction Fishing: Identifying discrepancies between ER records and follow-up specialist evaluations.
Quantifying Future Care and Long-Term Disability
High-value personal injury cases, particularly those involving catastrophic injuries, hinge on documenting permanency and projected care needs. Records must extend beyond historical treatment to include expert projections of long-term limitations and ongoing medical costs. This requires incorporating specialist evaluations from neurologists, orthopedic surgeons, or pain management experts who can credibly testify regarding the client’s future prognosis.
Effective medical record organization for PI cases ensures that expert witnesses receive a complete, structured file for review. Access to a well-organized medical history strengthens the expert’s opinion, making it more resistant to challenge during Daubert motions or at trial. This consistency is critical for demonstrating clinical documentation integrity in claims involving lifetime disability or anticipated surgical interventions.

Structural Best Practices for Record Integrity
- Comprehensive Collection: Obtain full treatment notes, including progress and therapy reports, not just billing summaries.
- Diagnostic Prioritization: Separate high-value objective findings (MRI, CT, lab results) from general care notes to highlight clinical significance.
- Causation Verification: Ensure physician notes explicitly connect the trauma to the current diagnosis, establishing liability and treatment necessity.
- Regular Auditing: Review records throughout recovery to identify missing files, correct errors, and maintain a complete chronology for litigation.
Beyond chronological accuracy, medical documentation in personal injury claims provides attorneys with actionable insights. A well-structured record not only proves causation and damages but also helps anticipate defense strategies, prioritize expert witness review, and identify potential gaps before they escalate. By integrating clinical findings with strategic case planning, firms gain a proactive stance, allowing them to negotiate settlements confidently while ensuring comprehensive representation for their clients.
At Social Surge Marketing, we focus on providing actionable insights and structured strategies for personal injury cases. Drawing from years of experience in managing complex medical documentation, our team assists law firms in organizing records effectively, ensuring every treatment note and expert evaluation is accounted for. By integrating clinical data with strategic review processes, we help legal teams anticipate challenges and maintain a strong position in negotiations.
Understanding how litigation-ready documentation affects case valuation is not just an academic exercise. By reviewing each file carefully, legal teams can anticipate defense arguments, highlight high-value evidence, and ensure that every aspect of injury and treatment supports the claim’s monetary potential.
In our experience, firms that implement rigorous medical record organization see smoother negotiations and stronger settlements. Even minor documentation gaps can become leverage points for adjusters, so attention to detail is critical.
Strategic Conclusion on Medical Case Evaluation
Applying medical record organization for PI cases ensures that a firm maintains full visibility into the treatment timeline, keeping legal strategy aligned with clinical realities. In complex cases, this operational discipline guarantees that every claim component is supported by verifiable documentation.
The core question, how medical records affect case valuation, ultimately comes down to clarity. A well-structured, chronological file removes ambiguity that insurers often exploit to reduce offers. Presenting a clean, objective record allows the legal team to secure a more accurate evaluation of damages.
A medical file’s structure is more than an administrative preference; it is a primary driver of case valuation. Organized, consistent, and objective records demonstrate causation, substantiate both economic and non-economic damages, and counter common defense tactics. This approach provides a clear roadmap for justifying future care costs and long-term disability claims.
For personal injury attorneys, maintaining rigorous standards in medical record organization is the most reliable way to achieve fair settlements. By integrating structured documentation into litigation strategy, legal teams protect client rights while supporting accurate, evidence-driven recovery projections, ensuring that every aspect of injury and care is fully represented.