In most personal injury cases, the strength of the evidence often determines whether a claim succeeds or fails during settlement negotiations. Among the most important forms of evidence are clinical records, which provide objective documentation of injuries, treatment timelines, and the long-term impact of an accident. Insurance adjusters, defense attorneys, and courts rely heavily on medical evidence when evaluating the credibility of an injury claim and the compensation it may justify.
Although medical documentation plays a critical role in proving liability and damages, it does not always strengthen a personal injury claim. Documentation problems such as missing records, inconsistent physician notes, or delays in treatment can weaken the legal argument supporting the case. When documentation issues appear, insurance adjusters often use them to question the legitimacy of the injury or reduce the settlement value.
For this reason, attorneys handling injury claims must carefully review clinical records and treatment documentation throughout the litigation process. Well-organized records can clearly demonstrate how an injury occurred, how it affected the victim, and why compensation is justified. Conversely, poorly structured or incomplete records can create doubt about causation and damages.
Understanding how medical records affect injury claims is essential for attorneys, legal teams, and professionals involved in personal injury litigation. By identifying documentation issues early, legal teams can strengthen their case strategy and improve the likelihood of achieving a fair settlement.
The Role of Documentation in Personal Injury Cases
Clinical records serve as one of the most important forms of evidence in personal injury litigation. These records provide objective information about the injuries suffered by a patient, the treatments recommended by physicians, and the progression of recovery over time.
In most injury claims, proper documentation serves three primary purposes:
- establishing the existence of the injury
- demonstrating that the accident caused the injury
- documenting the medical treatment required for recovery
When these elements appear clearly in treatment documentation and clinical evidence, they create a consistent narrative connecting the accident to the injury. This narrative helps insurance companies evaluate the claim and determine an appropriate settlement value.
Clinical records may include several different types of documents, such as emergency room reports, physician treatment notes, diagnostic imaging results, and physical therapy documentation. Each record contributes to the overall medical history of the injury.
However, when documentation is incomplete or inconsistent, the credibility of the claim may be questioned. Documentation issues in PI litigation can create uncertainty about when the injury occurred or whether the treatment was medically necessary.
Common Documentation Issues in PI Litigation
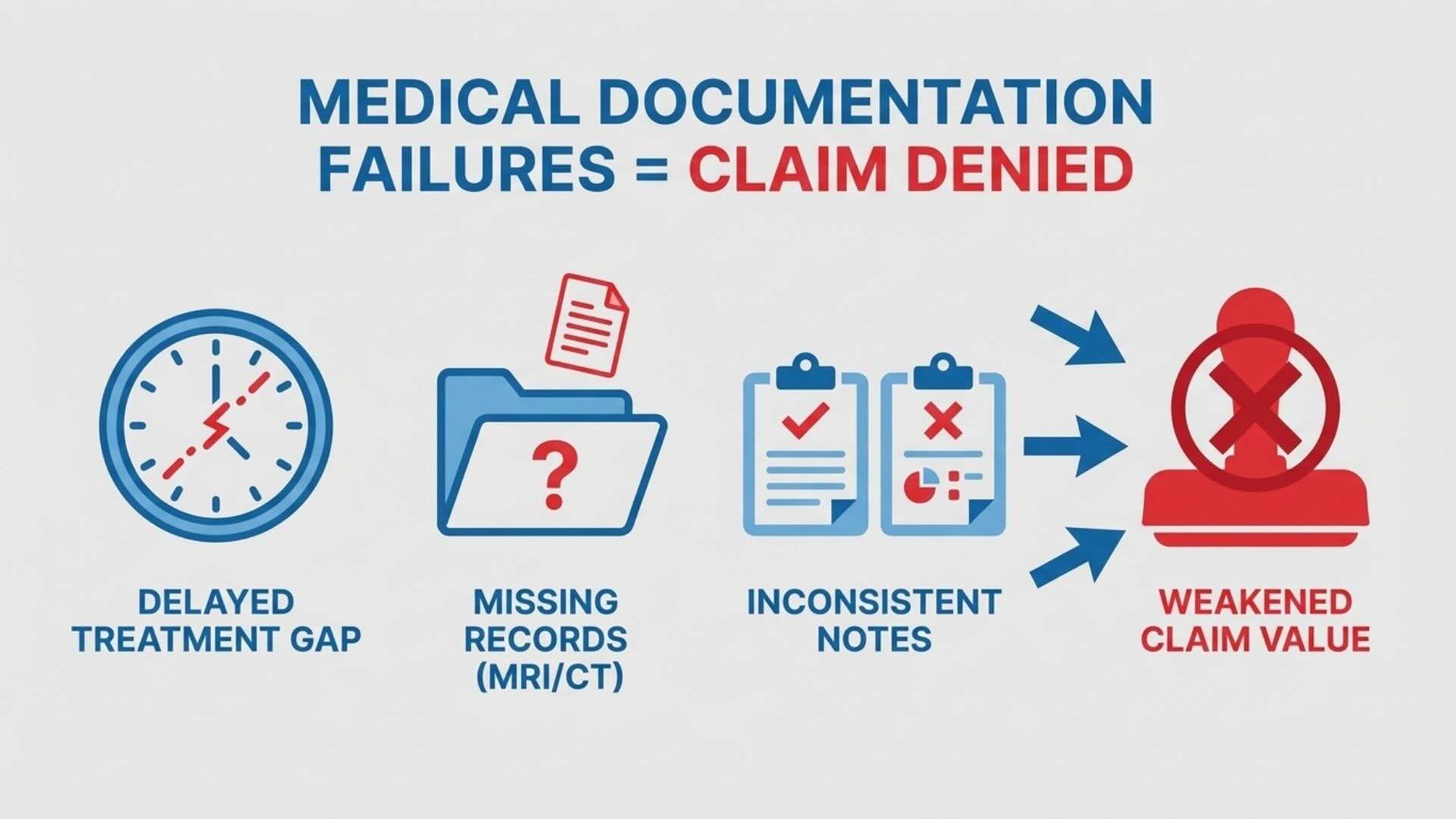
Common documentation problems in personal injury cases typically include:
- delayed medical treatment after an accident.
- missing diagnostic reports such as MRI or CT scans.
- inconsistent physician notes across different healthcare providers.
- gaps in the medical treatment timeline.
Many claims encounter documentation problems in injury cases because medical treatment often involves multiple providers and record systems. When these issues appear in clinical records, insurance companies may question whether the injury is directly related to the accident.
Delayed Medical Treatment
One of the most common documentation issues occurs when an injured person delays seeking medical care after an accident. Insurance companies frequently argue that a delayed treatment personal injury claim indicates that the injury was not serious or may not have been caused by the accident.
For example, if a patient waits several weeks before visiting a physician, insurers may claim the injury occurred later or resulted from another activity. Defense attorneys often argue that delayed treatment suggests the symptoms were unrelated to the original accident. Immediate medical evaluation helps create a clear timeline linking the accident to the injury.
Prompt treatment also allows physicians to document symptoms while they are still closely connected to the accident.
Missing or Incomplete Medical Records
Another common issue involves missing documentation. Personal injury treatment often involves several healthcare providers, including emergency departments, specialists, physical therapists, and diagnostic imaging facilities.
If records from any provider are missing, the medical documentation may appear incomplete. This is a frequent problem in missing medical records personal injury cases.
Examples of missing documentation:
- diagnostic imaging reports such as MRIs or CT scans
- specialist consultation reports
- rehabilitation or therapy records
Missing records can create gaps in the treatment timeline, making it more difficult for attorneys to demonstrate the full impact of the injury.
Medical Record Inconsistencies
Different healthcare providers may document injuries in slightly different ways. While these differences may be medically insignificant, insurance adjusters may interpret them as inconsistencies.
For example, one physician may describe an injury as moderate while another provider may describe it as mild. These inconsistencies can raise questions about the severity of the injury or the necessity of certain treatments.
Legal teams must carefully review medical records to identify potential inconsistencies before settlement negotiations begin.
How Medical Records Affect Injury Claims
Insurance companies rely heavily on clinical records and medical evidence when evaluating personal injury claims. In many cases, the strength of the documentation directly influences the value of the settlement. Adjusters analyze patient treatment records to determine whether the documentation supports the damages claimed by the plaintiff.
Insurance adjusters typically evaluate several factors:
- Treatment timeline: Consistent medical visits shortly after the accident demonstrate a strong connection between the incident and the injury.
- Diagnostic findings: Imaging results like MRIs, CT scans, and X-rays provide objective confirmation of injuries.
- Physician notes: Detailed documentation of symptoms and treatment recommendations shows how the injury affected the victim’s mobility, pain levels, and daily activities.
Understanding how medical records affect injury claims is crucial for legal teams. When these elements are clear, they strengthen the credibility of an injury claim and justify higher settlement values.
Why Insurance Companies Focus on Documentation
Insurance companies closely examine medical documentation because it often provides the most measurable evidence in an injury claim. Adjusters are trained to identify patterns suggesting exaggeration, unrelated injuries, or unnecessary treatment.
Documentation issues that attract attention include:
- large gaps between medical visits
- treatments appearing unrelated to the injury
- inconsistent physician descriptions of symptoms
Many law firms conduct structured reviews of medical documentation before settlement negotiations. Careful analysis allows attorneys to identify weaknesses and gather additional records when necessary. In many cases, medical record review for personal injury cases helps legal teams organize documentation, strengthen evidence, and improve claim credibility.
Preventing Documentation Problems in Injury Cases
Because documentation issues can weaken personal injury claims, attorneys and legal teams often take proactive steps to ensure that medical records remain accurate and consistent.
One effective approach is to monitor the client’s medical treatment throughout the life of the case. When attorneys track treatment progress, they can identify missing records or inconsistencies before negotiations begin.
Several practices can help prevent documentation problems.
- encouraging injured clients to seek medical care immediately after an accident
- ensuring consistent documentation across multiple healthcare providers
- collecting diagnostic reports and specialist evaluations early in the case
Legal teams may also rely on structured coordination services that help maintain organized treatment documentation throughout the litigation process. In complex cases, treatment oversight coordination for injury cases allows attorneys to track ongoing medical care, maintain consistent documentation, and ensure that treatment records remain aligned with the legal strategy of the case.
The Role of Expert Witnesses in Personal Injury Cases
In complex personal injury cases, expert medical witnesses often play an important role in interpreting medical documentation. These experts review medical records and provide professional opinions about the severity of the injury and the relationship between the accident and the documented treatment.
Expert testimony can help clarify medical record inconsistencies or explain complicated medical findings. In many cases, expert analysis strengthens the credibility of the medical evidence presented during settlement negotiations.
If you want to explore how documentation weaknesses can affect the strength of an injury claim, you can read our related article here: https://socialsurgemarketing.us/documentation-weaknesses-defense-attorneys-exploit/
This article explains how gaps, inconsistencies, or incomplete medical records can create challenges during personal injury litigation and how attorneys address these issues when building a strong case.
Conclusion
Medical records and clinical documentation play a central role in personal injury litigation. Clear and consistent records help establish causation, demonstrate damages, and support settlement negotiations.
However, documentation issues can weaken even valid claims. Delayed treatment, missing records, and medical record inconsistencies may create uncertainty about the legitimacy of the injury or the necessity of treatment.
Proper review addresses medical documentation weaknesses in PI cases and ensures claims are supported by credible evidence. Maintaining accurate records and consistent documentation significantly strengthens negotiation leverage during settlement discussions.